The anabolic steroid family tree is a framework that simplifies how different steroids impact muscle building and performance.
In general, the most commonly used anabolic steroids fall into one of three different families/categories.
Testosterone and its derivatives, Dihydrotestosterone (DHT) and its derivatives, and Nandrolone (19-Nortestosterone) and its derivatives.
Expectedly, many of the anabolic steroids in each family have similar attributes to one another.
There are exceptions to this in each family, but in general breaking down anabolic steroids into the three families provides a simplified framework to identify the targeted action of each compound, as well as how they impact muscle building and overall performance.
How Anabolic Steroids Enhance Muscle Building And Performance
There are countless processes in the body that are enhanced or inhibited by anabolic steroids.
To avoid overcomplicating this article with minutia, I will provide a bird’s-eye view of the main mechanisms that drive athletic performance or muscle building via exogenous anabolics.
When choosing which anabolic agents are most conducive to an athlete’s goals the following mechanisms should be taken into consideration, and compounds that are more heavily levered towards the desired effects should be favored.
- Anabolic activity via androgen receptor activation, aromatization, 5α-reduction, or the downstream conversion into metabolites that facilitate increases in muscle size and strength
- Antagonism of glucocorticoid receptors leading to the inhibition of protein breakdown and a net increase in muscle size and strength via muscle sparing
- Psychoactive effects in the brain leading to stronger training and subsequent increases in muscle size
- Stimulation of Erythropoietin (EPO) production leading to improved aerobic performance
When you start going down rabbit holes of how different anabolics impact different functions in the body outside of the basic understanding that drugs = results, it can become very overwhelming to make heads or tails of what the optimal protocol choice is for your personal goals.
At a higher level, even once you generally understand what compound choices would be wise just based on your goals, you will soon realize afterwards that you also have to factor in your tolerance of side effects with specific compounds, your current state of health, your age, your history of performance enhancing drug use, and a myriad of other factors.
Wise compound selection to maximize performance varies widely between different sports.
For example, an optimized protocol for a bodybuilder will likely be completely different than an optimized protocol for a MMA fighter.
This article will serve as an overarching introduction to how each category can be leveraged in the anabolic steroid family tree, as well as the general approach I would take towards compound selection.
Testosterone And Testosterone Derivatives
Testosterone is the parent hormone of this part of the family tree, and is also technically the parent hormone of the entire anabolic steroid family tree because DHT and Nandrolone are both derived from Testosterone.
Among Testosterone, the most notable Testosterone derivatives used for performance enhancement in this family are as follows:
- Testosterone
- Equipoise (Boldenone)
- Dianabol (Methandrostenolone)
- Halotestin (Fluoxymesterone)
- Turinabol (Chlorodehydromethyltestosterone)
The three compounds from this family most commonly used in a bodybuilding context are Testosterone, Boldenone (Equipoise) and Dianabol.
These three compounds are characterized mainly by their broad spectrum effects on anabolic and androgenic dependent functions, as well as their interaction with aromatase.
They all have strong influences on red blood cell count, energy systems, and exhibit a hybrid of behaviors in the body analogous to how endogenous steroidogenesis would otherwise regulate balanced activity.
They are anabolic, but not wildly so.
In general, this class of compounds facilitates a middle ground level of muscle growth, neurological effects, and enhancement of aerobic mechanisms.
Testosterone and Dianabol are both substrates for aromatase and can be enzymatically metabolized into potent estrogens.
Testosterone can be metabolized into Estradiol (E2), and Dianabol can be metabolized into Methylestradiol (17α-methylestradiol).
Boldenone’s level of estrogenicity is less clear as there is no solid data available that provides details on its interaction with aromatase in humans.
It has been stated that Boldenone is a less potent substrate for aromatase and is enzymatically metabolized into Estrogen at 50% of the rate of Testosterone.
This claim is not supported in any of the clinical data I have personally seen, so I would be hesitant to assume that Boldenone can facilitate sufficient Estrogen receptor activation in practical application as the base of a cycle.
There is also speculation around whether or not certain Boldenone metabolites act as aromatase inhibitors and attenuate the estrogenic activity of the parent hormone.
While this is certainly possible and warrants further research before we can make any conclusive statements about Boldenone, in general with our knowledge to date it is fairly well accepted in the community that Boldenone is mildly estrogenic, but significantly less so than Testosterone and Dianabol.
Halotestin and Turinabol are not substrates for aromatase so Testosterone, Dianabol and Boldenone are the only compounds in this section of the anabolic steroid family tree that can fill the role of a “Test base” and be used as the foundation of a steroid cycle.
Unlike the main three hormones used among bodybuilders in this family, Turinabol and Halotestin are Testosterone derivatives that induce effects analogous to potent DHT derivatives.
These two anabolics were chemically designed to lack estrogenic activity and a capacity to drive significant gains in mass, and be levered more towards pure protein expression and the neurological side of the spectrum.
Dihydrotestosterone (DHT) And DHT Derivatives
The next family in the anabolic steroid family tree is Dihydrotestosterone (DHT) and DHT derivatives.
DHT is the 5α-reduced metabolite of Testosterone that facilitates sexual differentiation of the male genitalia during embryogenesis and drives the maturation of boys into men during puberty.
It is much more androgenic than Testosterone, and sufficient amounts of it in androgen dependent tissues is necessary during puberty to ensure full maturation is achieved.
A common misconception is that steroids derived from DHT are guaranteed to be extremely androgenic simply because they are DHT derivatives.
On the contrary, DHT derivatives are almost all more tissue selective than Testosterone.
In general, all anabolic steroids were designed with that exact goal in mind, not just DHT derivatives.
Anabolic/androgenic ratios were evaluated in preclinical animal models before transitioning to human use in a clinical setting.
If a steroid did not exhibit a more favorable anabolic/androgenic ratio than Testosterone, it would have been abandoned for any application other than pure androgen replacement in males (e.g. Proviron).
The DHT derivatives most commonly used for performance enhancement include the following:
- Masteron (Drostanolone)
- Primobolan (Metenolone)
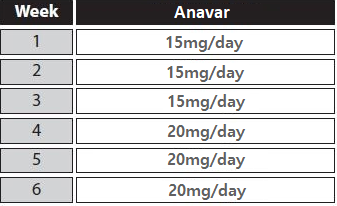
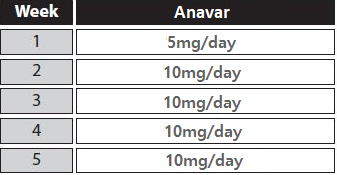
- Anavar (Oxandrolone)
- Anadrol (Oxymetholone)
- Winstrol (Stanozolol)
- Proviron (Mesterolone)
- Superdrol (Methasterone)
- DHB (Dihydroboldenone, 1-Testosterone)
DHT derivatives are often perceived to be poor choices for a mass building phase/offseason because they don’t seem to produce as much hypertrophy as the Testosterone and 19-Nor families.
This is another misconception, as DHT derivatives simply have more targeted action in the body.
They are not substrates for aromatase like Testosterone derivatives, they don’t act as potent agonists of a myriad of different receptors in the body like 19-Nors, and they don’t 5α-reduce into more androgenic metabolites.
DHT derivatives weed out a lot of the less predictable activity associated with the other two families and skew more towards pure protein expression and increased force production.
There is no water retention, there are no progestogenic side effects, all you get is pure muscle growth and proportionally higher amounts of strength gains relative to Testosterone Derivatives and 19-Nors.
DHT derivatives more or less exhibit targeted action on contractile tissue, which is why they’re commonly perceived to be “weak” anabolics, when in reality it is the lack of perceived side effects being misinterpreted as “weak.”
When it comes to nitrogen retention, we’ve seen in clinical studies that there is not a significant difference between the most potent steroids from each category of the anabolic steroid family tree.
“After 1935 the best method of discovering and measuring the protein-building action of androgenic steroids in humans proved to be metabolic balance studies.
In 1955, when anabolic steroids with less androgens were developed, the nitrogen-balance method was used again to evaluate and compare the nitrogen-sparing effect of the various preparations.
The findings of the numerous balance studies that were performed are as follows: The injectable 17 beta-esters, such as nandrolone phenylpropionate, nandrolone decanoate and methenolone enanthate exert a strong anabolic action for several weeks, amounting to 2-2.50 g nitrogen/day, which corresponds to a daily gain of 12-15 g protein or 60-75 g lean body mass.
The orally active 17-alkyl derivatives induce a dose-dependent nitrogen-saving effect of the same order.”
Nitrogen retention was roughly the same between all of the steroids evaluated in the study above.
It is more often than not the side effects themselves that are misinterpreted as one compound being more potent than another in a muscle building context.
If you gain 5 pounds of pure water retention in a week from using Dianabol, is it a more potent muscle builder than Anavar?
No, it’s not.
When everything is said and done, the amount of actual contractile tissue gained will be similar, but what happens to the body and how other mechanisms are augmented during that time span of you getting from point A to point B is what will differ significantly between those two compounds.
Just because DHT derivatives have more targeted action, it doesn’t mean that they are the ideal choice in all scenarios.
In fact, sometimes the side effects of certain compounds produce more desirable outcomes, depending on the goal.
In general, DHT derivatives are dry strength builders with reliable and predictable levels of anabolic activity.
An example of a sport where DHT derivatives are especially useful is MMA.
Fighters need to fight at as low of a weight class as possible without compromising their performance, they need to have a favorable ratio of force production relative to their body weight, and they also benefit greatly from increased aggression and neurological enhancement.
That is a specific scenario where using something that is skewed more towards the accrual of mass and less androgenic activity would be the worst choice.
For example, Nandrolone is 5α-reduced into DHN, a much less androgenic metabolite, and it also interacts with Progesterone receptors in the body which can have an anti-androgenic effect on the body.
While that might be a compound ideal for someone seeking maximum hypertrophy with a relative lack of androgenic side effects like hair loss, in this scenario the opposite is what we would be shooting for.
For a MMA fighter we want high force production and aggression with a relative lack of weight gain.
This is an example of a scenario where a DHT derivative would be wise to plug in.
Alternatively, that is an example of a scenario where Turinabol or Halotestin would be good options too, but that is only because they behave more like DHT derivatives than they do like Testosterone derivatives.
There are exceptions to the rule in every category of the anabolic steroid family tree, and the DHT derivatives are no different as they have Anadrol.
Despite being a DHT derivative, Anadrol behaves more like a 19-Nor as it drives significantly more pronounced gains in sheer mass (not to be confused with lean muscle mass) than the other DHT derivatives, and it is also an agonist of Estrogen receptors.
In general though, the DHT derivatives that are most commonly leveraged by athletes are Primobolan, Masteron, Anavar and Winstrol, and they all share similar overlapping effects on body composition and performance.
Nandrolone (19-Nortestosterone) And 19-Nortestosterone Derivatives
The last family in the anabolic steroid family tree is Nandrolone (19-Nortestosterone) and 19-Nortestosterone derivatives.
Many don’t even realize that Deca and NPP are not different drugs, and aren’t even representative of the actual drug their respective esters are attached to.
When someone refers to “Deca” they are referring to Nandrolone with a decanoate ester.
When someone refers to “NPP” they are referring to Nandrolone with a phenylpropionate ester.
The parent hormone of this family is Nandrolone (19-Nortestosterone), and all of the anabolic steroids in this category are Nandrolone derivatives.
Nandrolone derivatives are most commonly referred to simply as “19-Nors” in the bodybuilding community.
There are quite a few 19-Nors that have been synthesized and documented over the years, most of which are traditionally used at low dosages in women’s birth control.
The 19-Nors most commonly used for performance enhancement include the following:
- Nandrolone (19-Nortestosterone)
- Trenbolone (Trienolone)
- Trestolone (MENT)
19-Nors are generally characterized by their anabolism and progestogenic activity.
They are very anabolic, but they also exhibit significant amounts of satellite interaction with other receptors in the body.
The most notable being their interaction with the Progesterone receptor.
19-Nor derived progestins are agonists of the Progesterone receptor, which means that they can bind to the Progesterone receptor and activate it.
Nandrolone is not a potent substrate for aromatase, and mainly converts to a weaker Estrogen called Estrone (Estradiol is about 10-fold more potent than Estrone).
Nandrolone is also mildly estrogenic on its own via its ability to act as an Estrogen receptor alpha (ERα) agonist.
Overall, Nandrolone is much less androgenic and estrogenic than Testosterone.
Trenbolone is not a substrate for aromatase, however, some data suggests that it may interact with Estrogen receptors in a similar way to Nandrolone.
Trenbolone also facilitates superior muscle sparing via a handful of anti-catabolic mechanisms surrounding the glucocorticoid receptor.
Trenbolone binds to the glucocorticoid receptor and acts as an antagonist.
It also significantly suppresses glucocorticoid expression.
In addition, it lowers corticosterone and cortisol levels, while concurrently inhibiting cortisol from binding to skeletal muscle glucocorticoid receptors.
Through these mechanisms, Trenbolone exhibits a much more robust inhibition of muscle protein breakdown than Testosterone.
This is why Trenbolone seems to excel so much more than other anabolic steroids in a calorie deficit.
Trestolone (MENT) is unique from other 19-Nors in that it is a substrate for aromatase, and it behaves almost like a hybrid of a 19-Nor and Testosterone.
Because of this interaction with aromatase, Trestolone exhibits therapeutic promise as a potential HRT alternative, and may fill the role of a viable Test base alternative in a cycle.
The 19-Nors are the most suppressive family of the anabolic steroid family tree, and will keep your HPTA suppressed even at minuscule trace amounts.
Considering this, it would be prudent to reserve your use of them until you have decided if you will be blasting and cruising for the majority of your life.
Even one injection of Nandrolone can keep your HPTA suppressed for months, regardless of what you do.
The 19-Nor family skews more towards hypertrophy than the DHT derivatives, but is also accompanied by a myriad of satellite interaction with other receptors in the body that are less predictable and often warrant a more experienced user to responsibly manage.
19-Nors also have unique interactions with the GH/IGF-1 pathway that DHT derivatives don’t, which further complicates their responsible application, but can also be leveraged for increased levels of muscle growth in certain scenarios.
How To Determine Which Anabolics Are Optimal For Your Personal Goals
Understanding optimal applications of anabolics and side effect management can get very complicated, especially when you get into the weeds of sport specific applications, drug testing, lack of access to certain drugs, and budget limitations.
To simplify things, I highly recommend that you start your education on anabolic steroids by splitting them into the three families and working your way from the ground up.
Start in the Testosterone family and learn why a Testosterone base is used in the majority of enhancement protocols.
Delve into the mechanisms of Testosterone in the body, and how its aromatization into Estrogen and 5α-reduction into DHT facilitates a balancing act of anabolic and androgenic activity in the body, while simultaneously providing neuro and cardioprotection.
The majority of those reading this article will not have sport specific applications or drug tests they need to get around.
Considering this, the majority of you will be best served by learning about Testosterone thoroughly before even moving on to the other two families.
Testosterone is the bioidentical anabolic androgen we endogenously produce and rely on, and is more often than not the most intelligent hormone to use for a first cycle.
Only once you have fully leveraged the Testosterone family should you then move on to adding DHT derivatives in subsequent cycles.
If you have goals that cannot be met via Testosterone and DHT derivatives, or you experience undesirable side effects from Testosterone and/or DHT derivatives, then looking to the Nandrolone family would be warranted.
For a more elaborate explanation of how I would approach my first steroid cycle and each subsequent cycle thereafter if I could go back in time, I highly recommend you contact someone knowledgeable.
Don’t overwhelm yourself by trying to learn everything at once.
Learn about Testosterone and its derivatives.
Once you understand that family and know how to responsibly implement that information to achieve your goals, start learning about DHT derivatives.
Once you understand that family too and know how to responsibly implement that information to achieve your goals, start learning about Nandrolone and its derivatives.
Look, I totally understand this all can be quite overwhelming.. and you definitely don’t want to make mistakes where your body and health are concerned, so I again repeat… it is totally OK (and actually quite wise actually) to contact a more knowledgeable person on this subject. Someone who can guide you and make sure you are doing things right!
Here’s to your health.. and making great gains!